About LGMD2I/R9
LGMD is progressive and variable
Limb-girdle muscular dystrophy type 2I/R9 (LGMD2I/R9) is one of over 30 subtypes within a group of genetic muscle conditions that cause progressive muscle weakness, especially in the pelvic and shoulder muscle girdle. Symptoms often include extremity weakness, progressive leg weakness, and muscle wasting in the legs. Because each subtype is caused by a different genetic change, genetic testing is the only definitive way to confirm LGMD2I/R9.1,2
"Take a deep breath, because there is so much going on right now that is exciting...trials, research, and real progress for LGMD2I/R9 families."
–Melissa, an individual living with LGMD2I/R9

Mechanism of disease of LGMD2I/R9
Learn about the underlying genetic and biochemical mechanisms that cause LGMD2I/R9.
LGMD2I/R9 is rare and progressive
LGMD2I/R9 is a rare autosomal recessive disorder characterized by a progressive disease burden (eg, muscle weakness and mobility loss) and increased risk of cardiac and respiratory involvement compared with other LGMDs.3-5 There are approximately 7000 individuals with LGMD2I/R9 or other potentially addressable α-dystroglycanopathies in the United States and Europe.6*
*Includes all patients with potentially treatable mutations in FKRP, FKTN, and ISPD.


LGMD2I/R9 is commonly caused by pathogenic variants in the fukutin-related protein (FKRP) gene, with patients inheriting two copies of the mutated gene—one from each parent.4
The condition typically presents between childhood and early adulthood, with most individuals showing symptoms by age 18, often including limb weakness and early signs of muscle loss.7
Because LGMD2I/R9 can also affect respiratory and cardiac function over time, proactive care is an important part of managing this neuromuscular illness.1,5
LGMD2I/R9 weakens the structural integrity of muscle
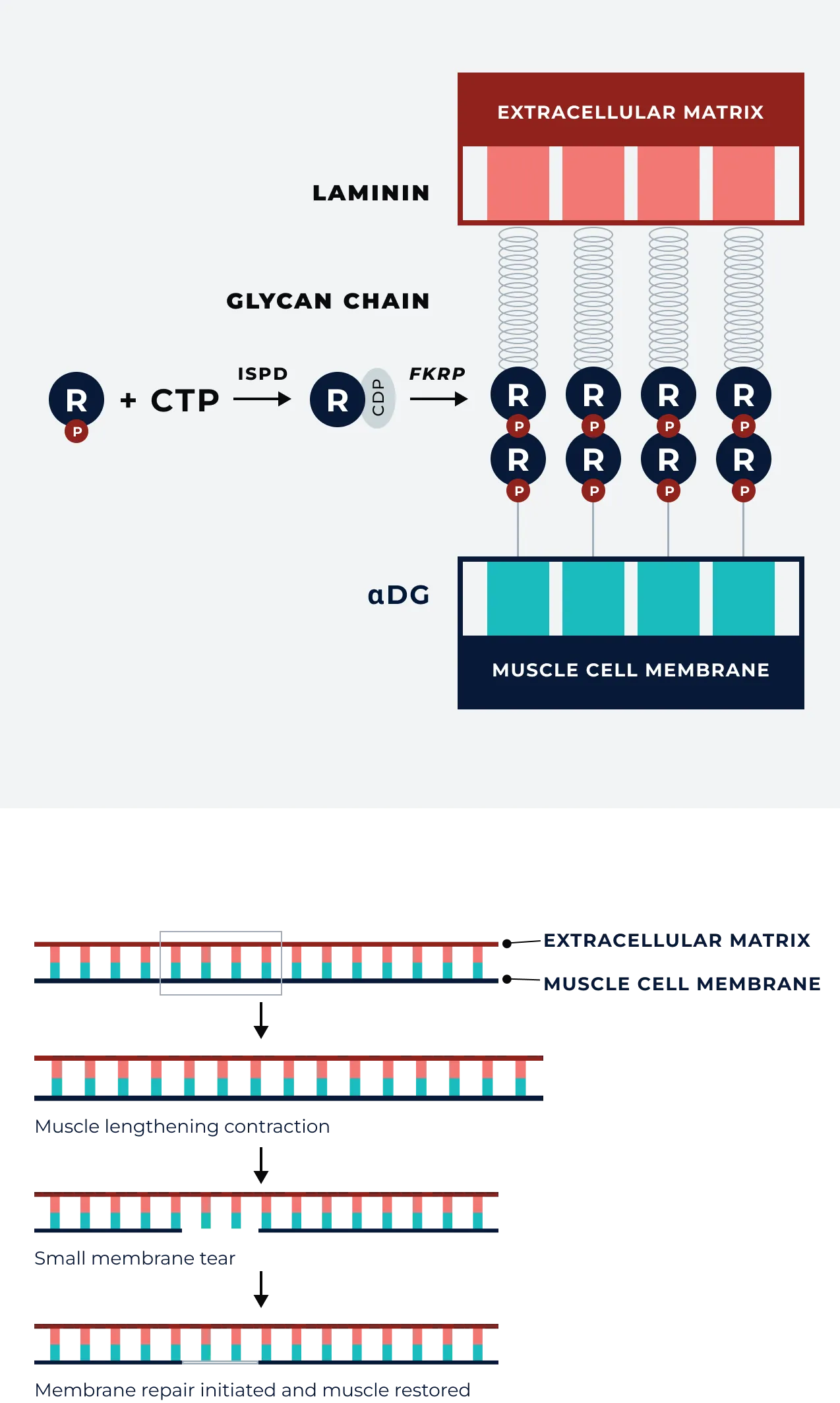
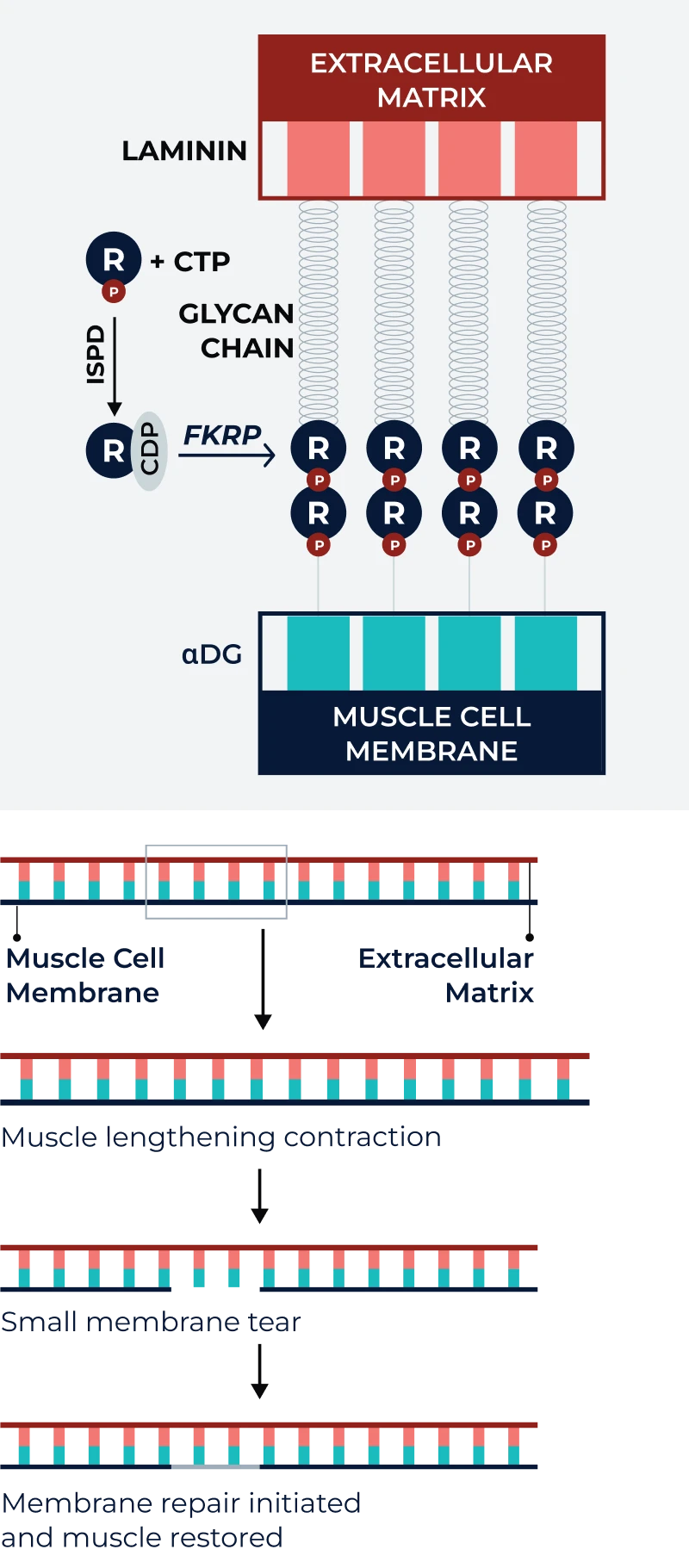
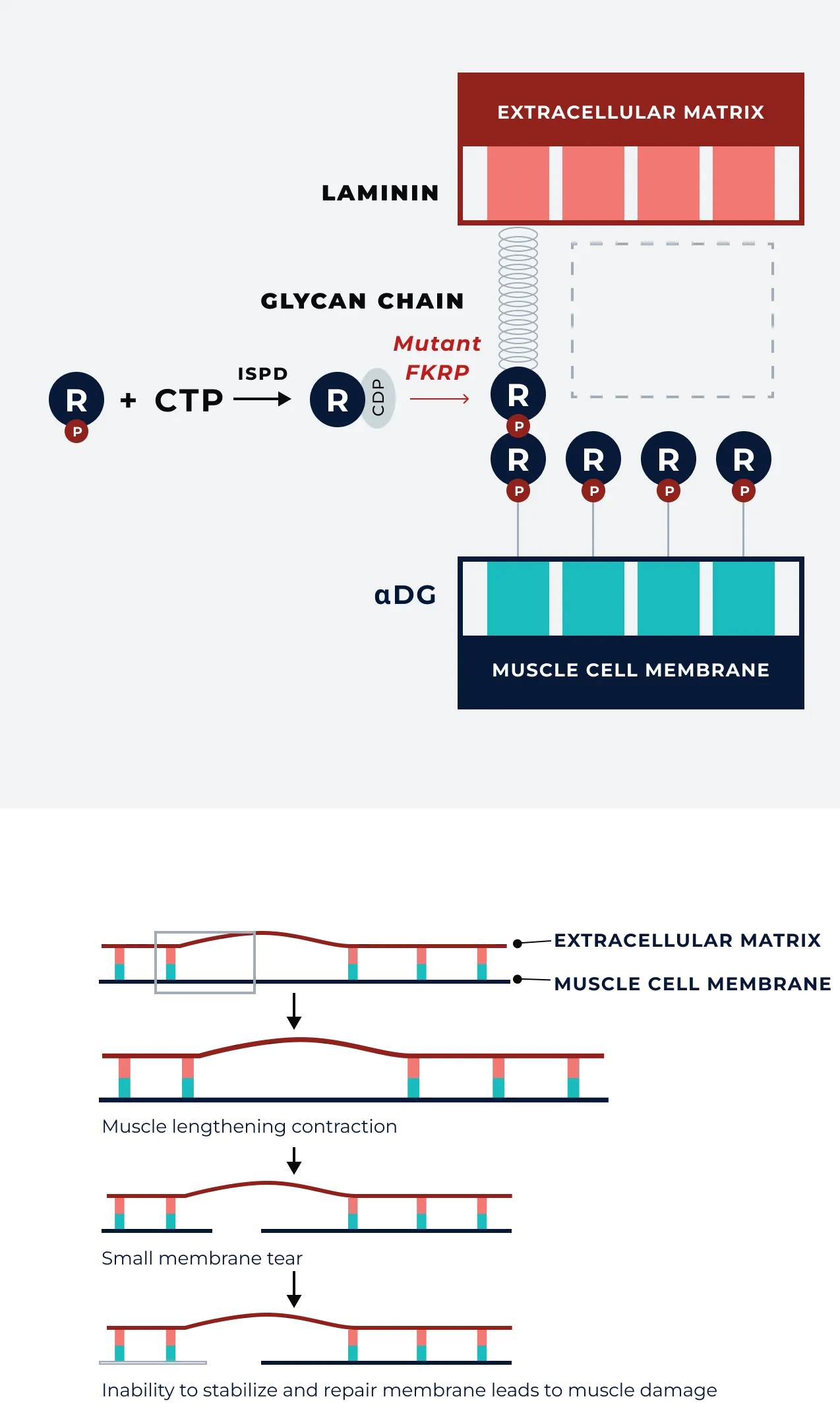
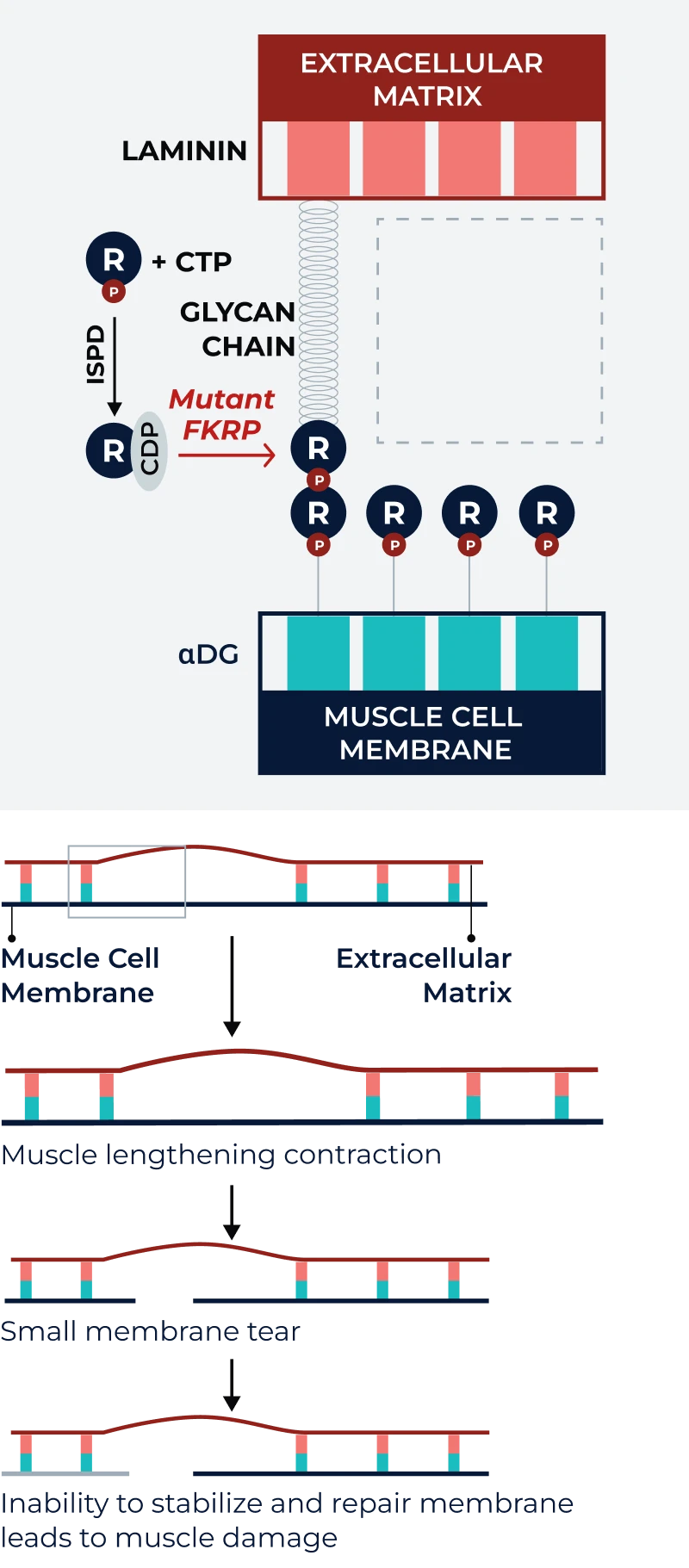
In LGMD2I/R9, the mutated FKRP gene, which codes for FKRP, an essential enzyme involved in the glycosylation of alpha-dystroglycan (αDG), results in defective glycosylation of αDG, leading to weakened muscle fibers and progressive degeneration.4,8,9
αDG plays a critical role in stabilizing muscle cells, a key component of the body’s biochemical shock absorbers that allows muscles to stretch, contract, and recover. This shock absorption system only works if αDG is glycosylated, and in individuals with FKRP mutations, the ability to glycosylate is impaired. Over time, this leads to inflammation and fibrosis of the muscle tissue, as well as muscle loss and failure. Eventually, individuals affected by LGMD2I/R9 may lose the ability to perform routine activities, such as walking or standing, without assistance.10-13
Healthy muscle tissue
LGMD2I/R9 muscle tissue
LGMD2I/R9 has an established genotype/phenotype association
Many FKRP mutations are associated with LGMD2I/R9, but homozygosity at c.826C>A (L276I) is common and always associated with LGMD2I/R9. Compared with individuals with other FKRP mutations, patients with L2761 homozygous tend to have relatively less severe disease, with a later onset of symptoms, lower rates of ambulation loss and wheelchair dependency, and a delayed need for respiratory support.14,15
HOMOZYGOTES (L276I/L276I)
- Symptom onset ~18 years old
- Lower limb & proximal weakness
- +/-calf hypertrophy, muscle pain, hyperCKemia
Loss of ambulation: 25% by age 40
Respiratory decline: Noninvasive assistance required by ~10% by age 40 and invasive assistance required by <1%
Cardiac dysfunction: ~30%
GENOTYPES (L276I/non-L276I) (non-L276I/non-L276I)
- Symptom onset ~5 years old
- Lower limb & proximal weakness
- +/-calf hypertrophy, muscle pain, hyperCKemia
- Lower limb & proximal weakness
- +/-calf hypertrophy, muscle pain, hyperCKemia
Loss of ambulation: Most by age 20
Respiratory decline: Invasive assistance required by 5% by age 39
Cardiac dysfunction: ~60%
- Symptom onset ~5 years old
- Lower limb & proximal weakness
- +/-calf hypertrophy, muscle pain, hyperCKemia
- Symptom onset ~18 years old
- Lower limb & proximal weakness
- +/-calf hypertrophy, muscle pain, hyperCKemia
- Lower limb & proximal weakness
- +/-calf hypertrophy, muscle pain, hyperCKemia
adulthood7,14,16
Loss of ambulation: 25% by age 40
Respiratory decline: Noninvasive assistance required by ~10% by age 40 and invasive assistance required by <1%
Cardiac dysfunction: ~30%
Loss of ambulation: Most by age 20
Respiratory decline: Invasive assistance required by 5% by age 39
Cardiac dysfunction: ~60%
CK=creatine kinase.